Echographie thyroïdienne
nodule EU-TIRADS 3 < 20 mm ou 4 < 15 mm => surveillance à 1a, puis 2-3a, puis 5a
| EU-TIRADS | Critères | Cytoponction | Malignité |
|---|---|---|---|
| 2 6% | anéchogène/spongiforme | compressif | 0% |
| 3 60% | iso/hyperéchogène | > 20 mm | 3% |
| 4 30% | modérément hypo | > 15 mm | 15% |
| 5 4% | très hypo, microCa, irrégulier, h>l | > 10 mm | 50% |
↗ taille significative +2 mm dans 2 diam. / 50% en volume => cytoponction
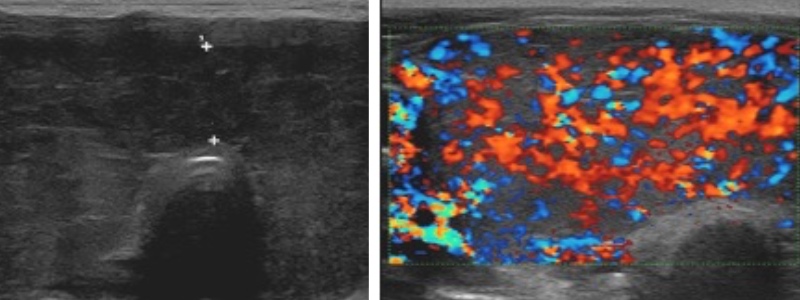
- goitre hypoéchogène homogène, Ac anti-récepteur de la TSH (TRAK)
- hypervascularisation intense > 1 m/s ("thyroid inferno" > 50% parenchyme)
- récidive : plus hétérogène et moins vascularisé
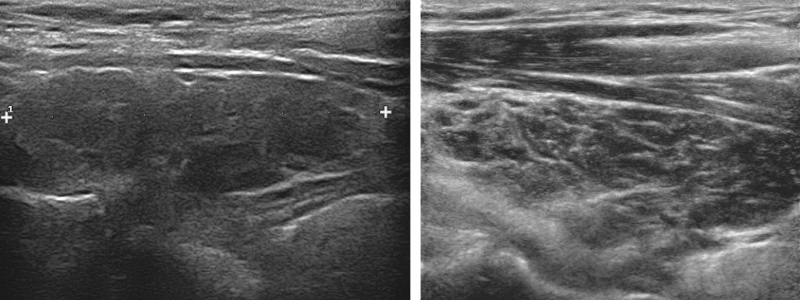
- goitre hypoéchogène micronodulaire, Ac anti-TPO +/- anti-Tg
- hypervascularisation modérée < 1 m/s
- suivi/an, travées fibreuses hyperécho, /!\ lymphome/cancer
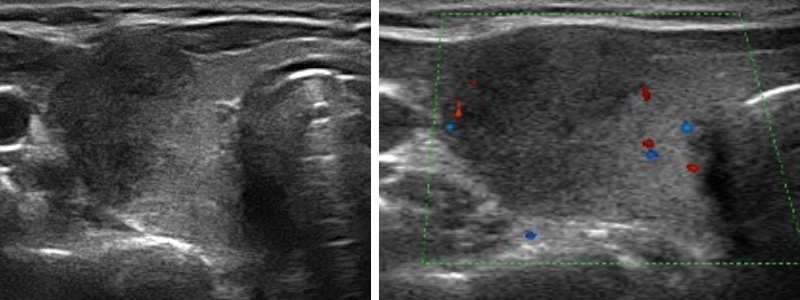
- contexte viral, douloureux
- plage hypoéchogène antéro-externe mal limitée peu vascularisée
- contrôle à M3 si pseudonodulaire
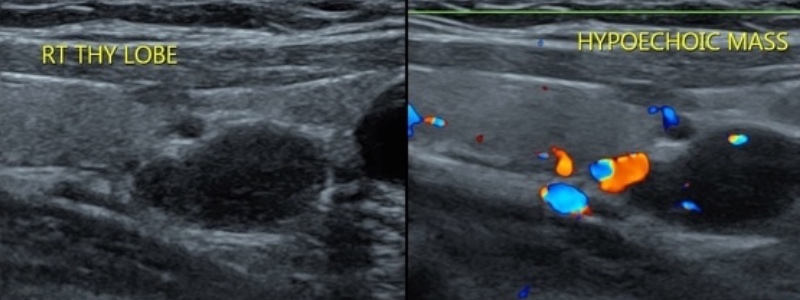
- 80% adénome parathyroïdien > 15% hyperplasie > 5% carcinome
- nodule hypoéchogène homogène > 1 cm + vascularisation
- à confronter à scintigraphie MIBI / TEP choline
| Bethesda | Signification | CAT |
|---|---|---|
| I | prélèvement non contributif | refaire des ponctions |
| II | bénin | surveillance à 1 an |
| III | indéterminé | surveillance à M6 ± ponctions |
| IV | tumeur vésiculaire ou oncocytaire | avis endoc (20% de cancer) |
| V et VI | suspect d'être malin et malin | chirurgie |